Definition
The term 'complex regional pain syndrome' or 'CRPS' was introduced in 1993
by the International Association for the Study of Pain (IASP) to more accurately
describe the pain syndromes reflex sympathetic dystrophy (type I), in which
injury occurs to the skin, bones, joints or tissue; and causalgia (type
II), in which injury occurs to major nerves. However, the clinical definition
and scientific understanding of this complex condition are still evolving.
'Regional' refers to the fact
that the pain is located in one region of the body (typically the hand or
foot); however, the condition can spread to additional areas.
Epidemiology
The actual incidence of CRPS is unknown. It is thought to be rare but
is often misdiagnosed.
The aetiology of CRPS is typically an injury: 16% after a fracture; 10-29%
after a strain or sprain;
3-24% post-surgery; 8% after contusion or crush injury; 6% spontaneous;
and 2%-17% due to other causes or of an unknown aetiology (Harden, 1999;
Allen, 1999). One report has estimated that CRPS develops in 1%-5% of
patients who have sustained peripheral nerve injury (type II) (Bonica,
1990). Despite treatment, many patients are left with varying degrees
of chronic pain
and disability. There are currently significant unmet medical needs for
patients suffering from CRPS.
Symptoms
Because CRPS affects the sympathetic nervous system, and this in turn
affects all tissue
levels (skin, bone, etc.), many symptoms may occur. The overriding symptom
is extreme
pain, either neuropathic or nociceptive, characterized as aching, burning,
pricking or shooting.
Other symptoms vary, but can include sensory changes (allodynia, hyperalgesia),
oedema, abnormalities of temperature, sudomotor activity and a change
in skin colour. The symptoms usually occur after an identified precipitating
event or trauma. Diagnosis depends on both
clinical findings and a detailed history. A confirmatory test is unavailable,
although a plain radiograph or a three-phase bone scan have been shown
to be useful. In addition, CRPS
has associated psychological sequelae. Because of continuous pain and
associated
disability, patients with CRPS may develop depression, anxiety and hypochondria.
Causes
The pathophysiology of CRPS is poorly understood. The theory that CRPS
is caused by
dysfunction of the sympathetic nervous system remains the subject of much
controversy.
A peripheral inflammatory component is also thought to play a role. The
condition can be
initiated by trauma, often involving the hands or feet. CRPS has also
occurred as an
iatrogenic complication after surgical procedures such as arthroscopy
and carpal tunnel
release. In addition, the syndrome has been reported after nerve injury
caused by intra-
muscular injection or routine venipuncture, and as an adverse reaction
to subcutaneous
allergy injections. CRPS has also been associated with medical conditions
such as diabetic
neuropathy, multiple sclerosis, myocardial infarction and cancerous infiltration
of a nerve
plexus.
Current treatments
Current guidelines recommend interdisciplinary management for CRPS, emphasizing
three
core treatment elements: pain management, rehabilitation and psychological
therapy. However, increasing evidence suggests that some cases are refractory
to conservative measures and instead require earlier intervention with
neurostimulation.
Conservative treatment
Rehabilitation: Rehabilitation is the cornerstone and first-line
treatment for CRPS. Mild cases
can respond to occupational therapy, physiotherapy and physical modalities.
These progress
from activation and isometric movement, to resisted range of motion (ROM)
and stress loading,
to ergonomics. A recent report of 103 children meeting IASP criteria showed
that 92% of patients experienced resolution or reduction of pain after
undergoing exercise therapy (Sherry, 1999).
Psychotherapy:
Psychological counselling and antidepressant drug therapy may be required
to treat the depression that is often associated with CRPS. Such therapies
have been shown to improve quality of life and to help develop pain-coping
skills and cognitive-behavioural psychotherapy. Psychotherapy can also
facilitate progress in the other treatment modalities.
Pharmacological management
and regional anaesthesia techniques
In those cases that are mild to moderate, and in which rehabilitation
is only partially successful, adjuvant treatment with drugs such as anti-inflammatories,
corticosteroids, antidepressants, anticonvulsants, calcitonin or opioids
can be administered. Patients often take several different drugs simultaneously
to maximise their pain relief. However, no single drug or combination
of drugs has been shown to produce long-lasting symptom relief.
Interventional pain
management
In those patients that develop refractory chronic pain, a multidisciplinary
approach is required
that includes other pain interventions in addition to conservative treatments.
Other pain relieving measures include sympathetic/somatic blockade, neurostimulation
and intrathecal drug delivery. Increasingly, neurosurgical methods are
becoming an indispensable part of the therapeutic armamentarium for treatment
of CRPS.
Minimally interventional:
Sympathetic nerve blocks involve injecting anaesthetic into different
nerves. These include stellate ganglion nerve blocks, lumbar sympathetic
nerve blocks and
Bier blocks. However, there is little clinical evidence to suggest that
sympathetic nerve blocks
are effective. Other minimally invasive block techniques include intravenous
(IV) regional blocks and somatic nerve blocks. These treatments have been
shown to provide immediate pain relief
for CRPS sufferers, but in many cases the effects are not long-lasting.
Furthermore, there is a
lack of prospective studies evaluating the clinical efficacy of these
treatments.
More interventional:
If patients fail to progress through the rehabilitative pathway, or have
inadequate or only partial pain relief, more interventional procedures
are used. Epidural and plexus catheter blocks may be considered if the
patient had a partial response to sympathetic
or somatic nerve blocks, although there is a lack of clinical evidence
to support their use.
The next step in the pain management pathway is neurostimulation.
Neurostimulation:
This therapy is increasingly replacing ablative pain surgery procedures.
Neurostimulation can be administered as either spinal cord stimulation
(SCS) or peripheral
nerve stimulation (PNS), although SCS is the standard practice. In one
study (Kumar, 1997), neurostimulation showed effective pain relief that
was superior to ablative surgery. Another
recent study showed that neurostimulation resulted in sustained pain control
in severe CRPS
type 1 sufferers with a probable reduction in narcotics (Kemler, 2000).
This study also showed
that neurostimulation provided significantly better long-term pain relief
compared with physiotherapy alone. A recent review suggests that SCS may
produce substantial and long-lasting pain relief in 60-70% of patients
(Meyerson, 2001). In addition, neurostimulation has also been found to
be less costly than standard treatment. A cost analysis model of patients
with CRPS
type I found that although at 12 months the mean cost of neurostimulation
per patient (9,352)
was more expensive than physical therapy (6,735), this difference
was reversed over a lifetime analysis, resulting in a cost saving with
neurostimulation (58,471). Given that SCS is both more effective
and less costly than conventional treatment, the authors concluded that
'there is compelling evidence for its adoption and appropriate utilization'.
This new evidence, in combination with the cost-effectiveness
of neurostimulation, suggests that this therapy is currently being underused.
Intrathecal drug delivery:
Intrathecal drug delivery can be used to treat CRPS patients who have
a significant component of dystonia, who have failed neurostimulation,
who have longstanding disease, who have multi-limb involvement or who
need palliative care. Patient selection appears
to be critical to success with intrathecal drug delivery for pain, and
suitable candidates can be easily established through a screening test.
This method of delivery reduces the opioid dose
that must be administered compared with systemic methods, with the consequence
that there
are fewer side effects. Two recent studies demonstrated the effectiveness
of intrathecal baclofen
in the treatment of CRPS-associated dystonia (van Hilten, 2000; Zuniga,
2002).
Surgery - sympathectomy
This highly controversial treatment involves the destruction of nerves
using surgery or chemicals, and is indicated only for profoundly disabled
patients who have responded positively to sympathetic blockade and have
no other treatment options. Evidence to support the use of sympathectomy
is limited, and as such its use is not widely recommended. Some retrospective
studies of surgical sympothectomy have shown long-term success (Schwartzman,
1997; Kim, 2002; Brandyk, 2002). However, these successful outcomes should
be balanced with reports
of the negative impact of surgical sympathectomy (Furlan, 2001).
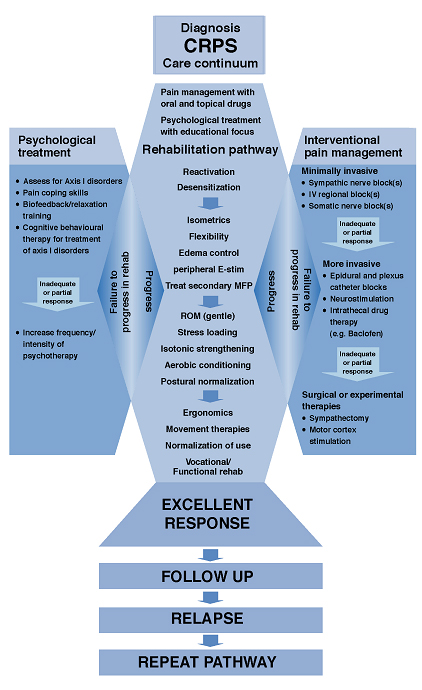
Interdisciplinary
clinical pathway
The goal of treatment is to improve function, relieve pain and achieve
remission using an interdisciplinary approach with simultaneous application
of rehabilitation, pain management
and psychological treatments. These modalities should be applied in a
timely manner, with advanced treatments applied according to the patient's
clinical response. Failure to progress
in the rehabilitation pathway requires more advanced pain management and
psychological approaches. The importance of criteria to define appropriate
patient selection in CPRS has
been recently highlighted.
CRPS patients generally respond to conservative
treatment including pharmacological management, whilst some patients may
experience short-term pain relief with nerve blocks.
When patients are refractory to conservative measures, flexible use of
neurostimulation (SCS) should be considered, based on each patient's clinical
progress. In addition, the interdisciplinary clinical pathway suggests
that SCS should be used earlier in CRPS patients who do not respond to
an acceptable level of treatment within 12 weeks (Stanton-Hicks, 2002).
This may be particularly beneficial for younger patients.
|